
 In the usually joyous Chinese New Year holiday season of 2020, anxiety was the mood as the novel coronavirus pneumonia epidemic spread across the nation. Wuhan and various surrounding cities in the Hubei province implemented traffic controls, and a total of 30 provincial-level administrative regions initiated a first-level major public health emergency response, introducing various epidemic control measures. But as the number of diagnoses increases, these measures were not sufficient to completely remedy the sense of panic among the public, writes James Liang, chairman and co-founder of trip.com.
In the usually joyous Chinese New Year holiday season of 2020, anxiety was the mood as the novel coronavirus pneumonia epidemic spread across the nation. Wuhan and various surrounding cities in the Hubei province implemented traffic controls, and a total of 30 provincial-level administrative regions initiated a first-level major public health emergency response, introducing various epidemic control measures. But as the number of diagnoses increases, these measures were not sufficient to completely remedy the sense of panic among the public, writes James Liang, chairman and co-founder of trip.com.
According to preliminary data, the novel coronavirus is relatively transmissible but has a lower mortality rate than SARS. Some infected individuals show no symptoms in the initial stage, and the most severe or fatal cases were those of elderly people with pre-existing conditions. These criteria are similar to the common cold. Novel coronavirus and influenza are both respiratory infections, though presenting different symptoms.

In view of the similarities between the novel coronavirus and influenza, a simple comparison between the epidemiological data of the two can be made. Due to differences in the standards for calculation and incompleteness of influenza data in China, data from the US Centre for Disease and Prevention Control (CDC) gives a more complete picture of the nature of influenza. The following data is based on professional data sampling and models, which is more stable and comparable between different years.
Table 1. Estimated impact of influenza in the US from the 2010-2011 flu season through to the 2018-2019 flu season
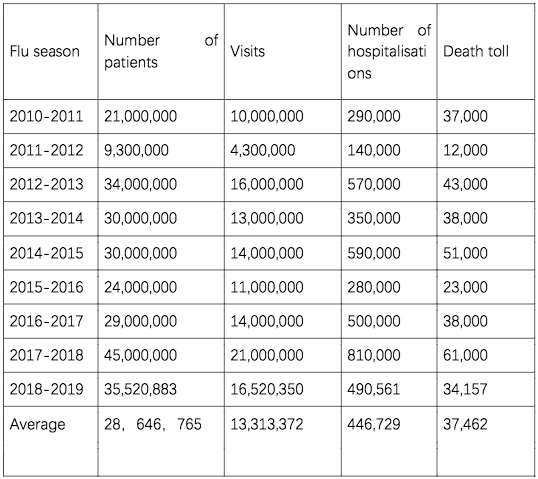
On the basis of the above statistics, we can calculate several rates for influenza in the US: Prevalence = number of patients / total U.S. population = 28,646,765 / 32 00 00000 = 9 % Mortality rate = deaths / sick persons = 37462 / 28,646,765 = 0. 13 % Hospital attendance rate = the number of visits / sick persons = 13,313,372 / 28,646,765 = 46 % Hospitalisation rate = number of hospitalisations / sick persons = 446,729 / 28,646,765 = 1.6 %
Compared to the latest statistics of the new coronavirus in China:
Table 2. Case data for the new coronavirus in and outside Hubei Province as of 27 January 2020
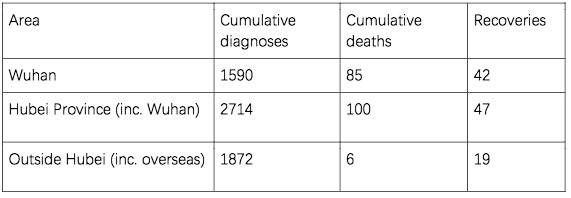
The key to estimating the toxicity of the novel coronavirus is the mortality rate. On the basis of publicly available data, the mortality rate can be estimated:
Mortality = deaths / sick persons Number of diagnoses = prevalence * rate of diagnoses
So, we can infer that:
Mortality rate = deaths / number of diagnoses * rate of diagnoses
For the data from outside of Hubei, we can infer that:
Mortality rate = 6 / 1872 * rate of diagnoses = 0.32% * rate of diagnoses
Assuming that outside of Hubei, 100% of hospital attendances result in a diagnosis of novel coronavirus, then the rate of diagnoses would be equal to the attendance rate. Estimating on the basis of the attendance rate 46% for influenza in the US, the mortality rate for outside of Hubei = 0.32% * 46% = 0.14%, while the mortality rate in the US for the past few years is 0.13%.
It should be emphasised that the above calculations are made on the basis of the data that is currently available. As the novel coronavirus epidemic continues to develop, in most cases reaching a peak in the second week, and infections outside of Hubei have been later than those within Hubei, with a currently very low rate of recovery, we cannot rule out the possibility that the mortality rate will experience a significant increase.
Let us examine the situation in Hubei

Mortality rate = 100 / 2714 * rate of diagnoses
= 3.68% * rate of diagnoses
Using the same rate of diagnoses of 46%, the mortality rate in Hubei is as high as 1.69%, far higher than the mortality rate outside Hubei. But it is inconceivable that the same illness could have such disparate mortality rates. It is more likely that the rate of diagnoses in Hubei is much lower than 46%, as Hubei does not have the capacity to diagnose sick persons. It is highly likely that the actual number of patients is far higher than the number of patients currently diagnosed, and that the mortality rate is far lower than this figure.
It is likely that the actual number of infections in Hubei is far higher than the number of diagnoses. In light of the fact that cases of morality have been preceded by severe symptoms leading to diagnosis, we can infer that the number of deaths in Hubei has not been underestimated. Therefore, the actual number of infection deaths in Hubei could be far lower than the above estimate.
“The actual rate of prevalence may be even lower than 3%”
Since the novel coronavirus has been spreading in Wuhan for a month or two, we can infer the number of infected individuals in Wuhan, assuming the prevalence of the novel coronavirus is the same as that of influenza in the US. The average prevalence of influenza in the US over the past nine years is 9%. If one-third of flu diagnoses are concentrated in the winter season, then 3% of the population will be infected. According to data from the Wuhan Statistics Bureau, Wuhan has a permanent population of 11 million. 3% of the population would thus be a formidable 330,000 infected individuals. But, on the basis of a 0.1-0.2% mortality rate, the number of deaths, similar to the common cold, will be 300-600. Of course, any death is a tragedy, but in US cities of the same size, the common cold causes a similar magnitude of impact. With the preventive measures of the government, the actual rate of prevalence may be even lower than 3%.
As there is no cure for influenza, for the majority of patients, the most effective treatment option is not hospitalisation, but to stay at home and rest. According to the figures for 2011- 2019, the hospitalisation rate for flu patients in the US is 1.6%. No city’s medical system could cope if all people expressing symptoms of the flu required hospitalisation, even possibly leading to a collapse of the medical systems. If panic levels intensify, and all patients with flu-like symptoms demand hospitalisation, the number of hospitalisations will be multiplied dozens of times, and cause great pressure on medical staff. Luckily, the Chinese government has expanded efforts to deliver relief to Wuhan, alleviating the local sense of panic through direct medical aid.
At present, Hospitals in Hubei and Wuhan do not have the capacity to receive such a massive number of suspected patients, leading to concern that not all infections are accounted for, and the rate of infection for influenza in the US seems to support this theory.
“The toxicity of the novel coronavirus can be determined to be similar to that of influenza”
However, if the number of deaths in Hubei does not significantly increase, even if the number of diagnoses in Hubei does increase, it can only be proven that the number of infections is higher than previously estimated. That is to say, with a higher number of infections, the mortality rate will be lower than estimated. Even if there is not an observable increase in the number of diagnoses, this could be attributable to the fact that those without symptoms or small infections have, as per advice, remained in isolation at home, and does not indicate that the infection mortality rate outside Hubei has been underestimated. Most importantly, so long as the mortality rate outside Hubei does not dramatically increase, the toxicity of the novel coronavirus can be determined to be similar to that of influenza in the US.
We can also draw a comparison between the mortality rate of the novel coronavirus and SARS. According to the World Health Organisation, as of 29 May 2003, the global number of cumulative cases for SARS was 8295, with 750 deaths and a mortality rate of 9.04%. It can be seen that, among the three communicable diseases of novel coronavirus, SARS and influenza, the mortality rate of the novel coronavirus is closer to influenza and much lower than SARS.
“Excessive hospitalisation…could serve to increase the risk of being infected”
Summing up, so long as the mortality rate does not experience a significant climb, even if the number of diagnoses will continue to increase, we can be cautiously optimistic that the epidemic can be controlled. Of course, we do not recommend relaxing preventative measures, we merely hope that this analysis will help to alleviate excessive panic.
The above analysis also supports the government’s recommendation for those without symptoms or small infections to remain in isolation at home. No country or city can afford to treat all patients expressing symptoms of the flu, and excessive hospitalisation as a result of panic could serve to increase the risk of being infected.
“We hope that governments… will adopt reasonable measures in responding to the outbreak”
It should be noted that the inferences of this article are based on the latest figures from books on influenza in the US. Importantly, if the number of death outside Hubei, including within China, remains low, the relatively optimistic speculation in this article could serve to relieve panic.
It is also possible that the zero mortalities outside Hubei, especially abroad, informed the 23 January 2020 decision by the World Health Organisation not to designate the outbreak as a public health emergency of international concern, and not to recommend travel and trade restrictions. We, therefore, hope that governments and companies abroad will adopt reasonable and appropriate measures in responding to the outbreak.
Comments are closed.